What is it?
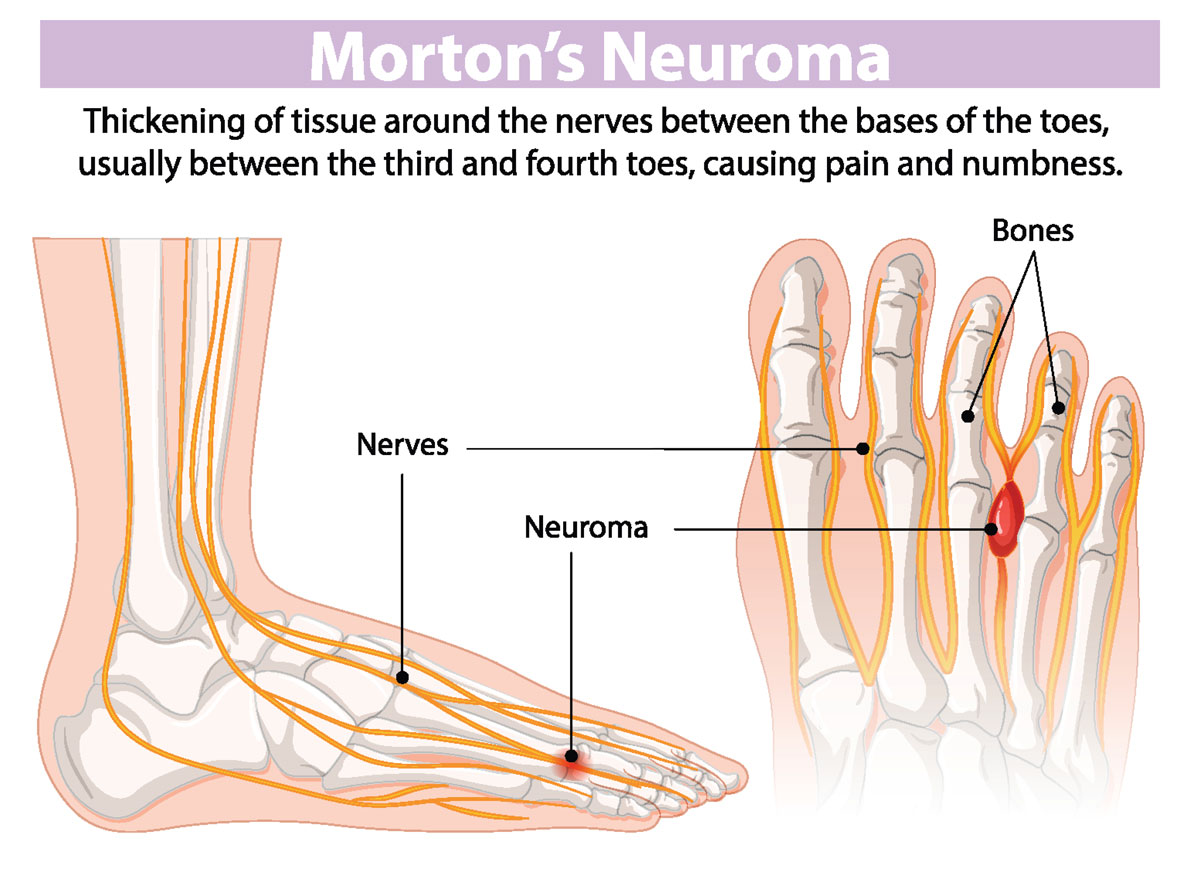
Morton’s neuroma is a benign but painful condition that affects one of the sensory interdigital nerves of the foot. It consists of a thickening and inflammation of the portion of the nerve that runs between the metatarsal heads, most commonly in the third intermetatarsal space (between the third and fourth metatarsals).
This condition usually develops in patients between the ages of 35 and 50, more frequently in women, especially those who regularly wear narrow shoes or high heels.
Causes of Morton’s Neuroma
The onset of Morton’s neuroma is typically due to multiple contributing factors:
- Anatomical: a reduced space between the metatarsals increases friction between the interdigital nerve and the bones.
- Postural: poor foot alignment or abnormal gait mechanics place excessive stress on the metatarsals.
- Footwear: prolonged use of tight shoes and/or high heels.
- Excess weight: added load increases forefoot pressure.
- Repetitive stress: common in certain sports or occupations requiring frequent forefoot loading.
- Trauma: direct or repeated injury to the forefoot.
Regardless of the underlying cause, the mechanism leading to neuroma formation is always the same: chronic mechanical irritation of the nerve by the metatarsal heads.

Symptoms of Morton’s Neuroma
Patients typically experience pain in the ball of the foot (forefoot), which worsens when wearing tight shoes and improves when barefoot. The pain is often described as burning and may be accompanied by numbness and tingling (paresthesia) in the toes.
Diagnosis of Morton’s Neuroma
In most cases, diagnosis is based on symptoms and the Mulder’s sign (pain and a palpable click when compressing the forefoot).
Because the symptoms may resemble other conditions, Morton’s neuroma can sometimes be mistaken for:
- Metatarsal capsulitis
- Bursitis or arthritis
- Stress fractures
- Metatarsal osteochondrosis (Freiberg’s disease, also known as Köhler’s disease type II)
To confirm the diagnosis, the physician may order imaging tests such as X-rays, ultrasound, or MRI.
Conservative Treatment of Morton’s Neuroma
When symptoms have been present for less than six months, conservative treatment is usually recommended. Approaches include:
Physical Therapy
Manual therapy and physical modalities such as high-power laser therapy can help reduce nerve compression and inflammation.
Orthotics
Custom or temporary shoe inserts may relieve pressure in the area of the neuroma.
Pharmacological Treatment (Cortisone Injections)
Corticosteroid and anesthetic injections can be administered directly at the site identified by ultrasound. The goal is to reduce inflammation and nerve thickening.
Limitations: The effects are often temporary. Pain may return, and repeated injections may weaken nearby tendons and ligaments.
Alcohol Sclerosing Therapy
This treatment involves injecting diluted alcohol into the neuroma to destroy the nerve sheath and eliminate pain. It is considered a valid alternative to cortisone and surgery.
Cryotherapy
The application of very low temperatures aims to interrupt nerve conduction and reduce pain. However, its effectiveness remains controversial.

Riva Method (causal Treatment)
The Riva Method focuses on addressing the root cause: excessive mechanical stress on the nerve during foot strike.
By improving single-leg stability through enhanced proprioceptive reflexes and activation of stabilizing muscles, along with structural remodeling of the foot that increases strength and load capacity, the method reduces nerve compression.
Within a few weeks, symptoms may disappear as inflammation and nerve thickening gradually regress. This is the only approach capable of breaking the vicious cycle of nerve irritation and promoting true functional recovery.
Surgical Treatment of Morton’s NeuromaIf conservative treatments fail, surgery may be necessary. The standard procedure is a neurectomy, which involves removing the affected portion of the nerve. In some cases, surgery may instead focus on creating more space around the compressed nerve by releasing scar tissue or nearby structures.