
What Is the Foot’s Role?
Your foot is much more than a structure for standing and walking. It’s a sensory organ that connects your body to the ground, helping you move safely and efficiently.
The human foot has:
- 26 bones
- 33 joints
- Over 100 ligaments
- Dozens of muscles
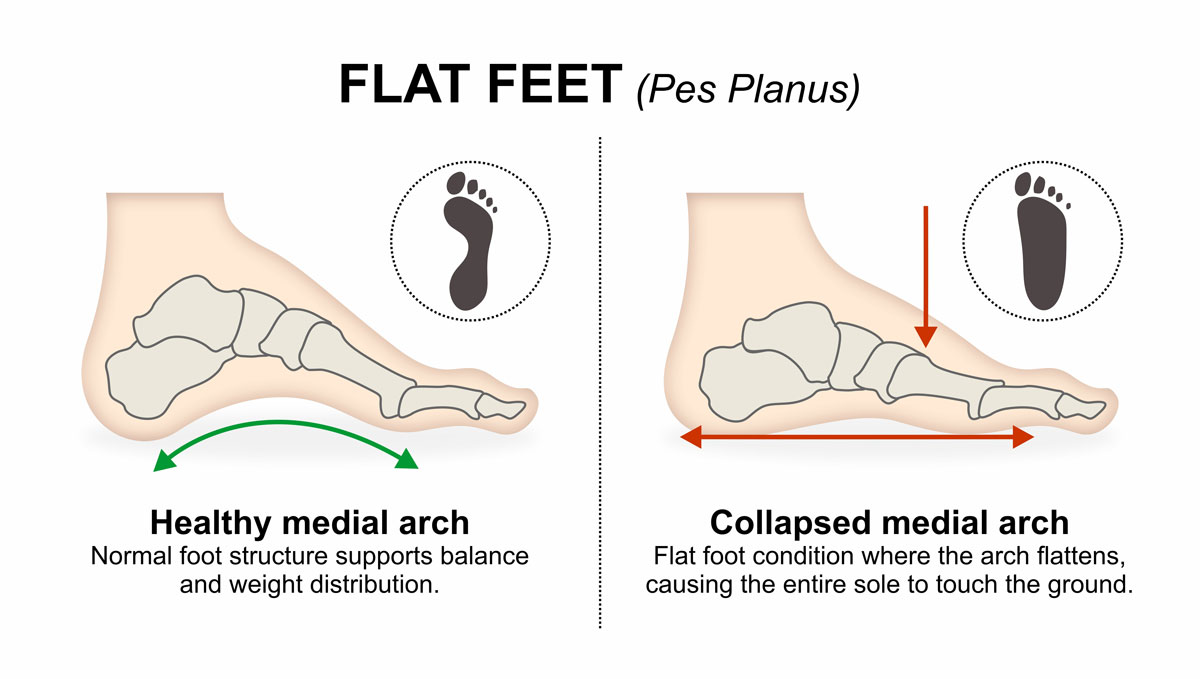
Along the inside of the foot is a raised area called the medial longitudinal arch. In flatfoot, this arch is lower than normal—or completely flattened—often accompanied by heel valgus, where the upper heel tilts inward relative to the lower leg.
Flatfoot in Children
- In children, the foot is naturally flat, which is generally considered physiological until the age of 8–10, followed by gradual maturation that ends around 10–12 years of age.
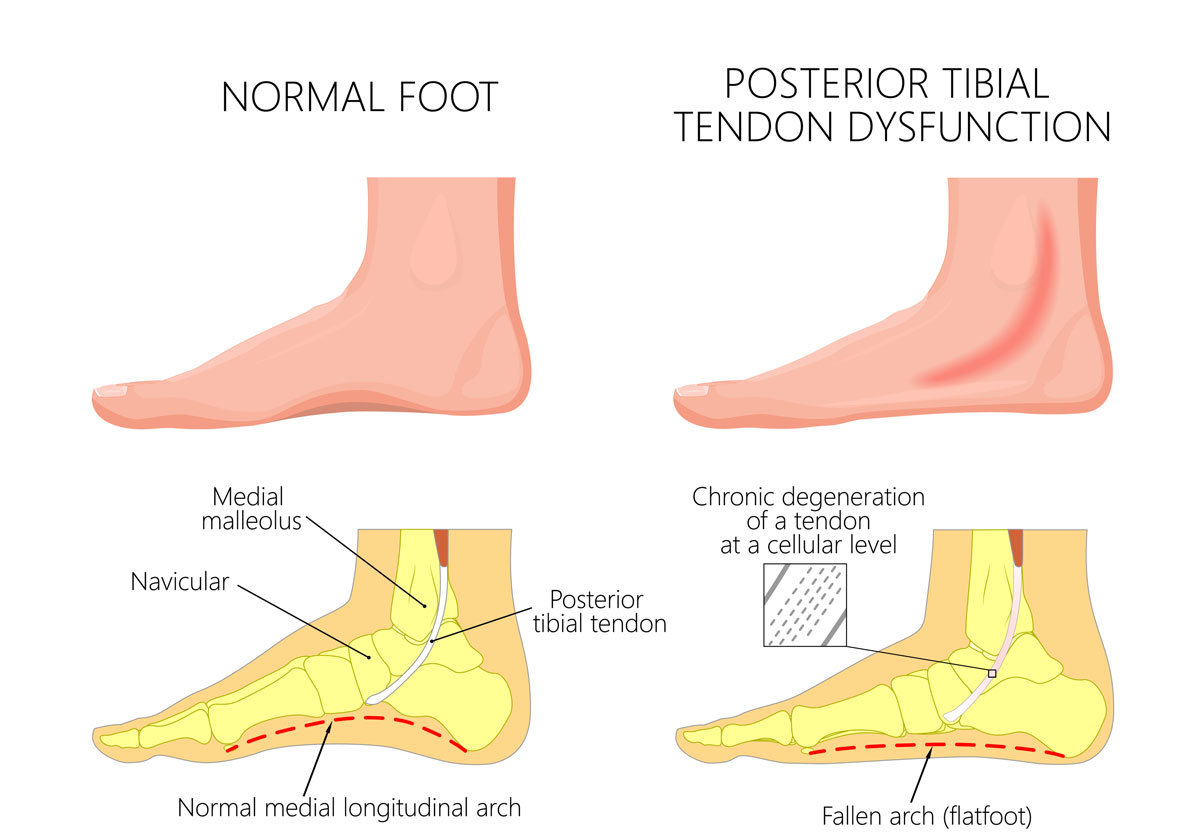
- Flatfoot happens when the talus bone “collapses” downward, the heel tilts inward, and the posterior tibial tendon is stretched trying to support the arch.

Causes of Flatfoot
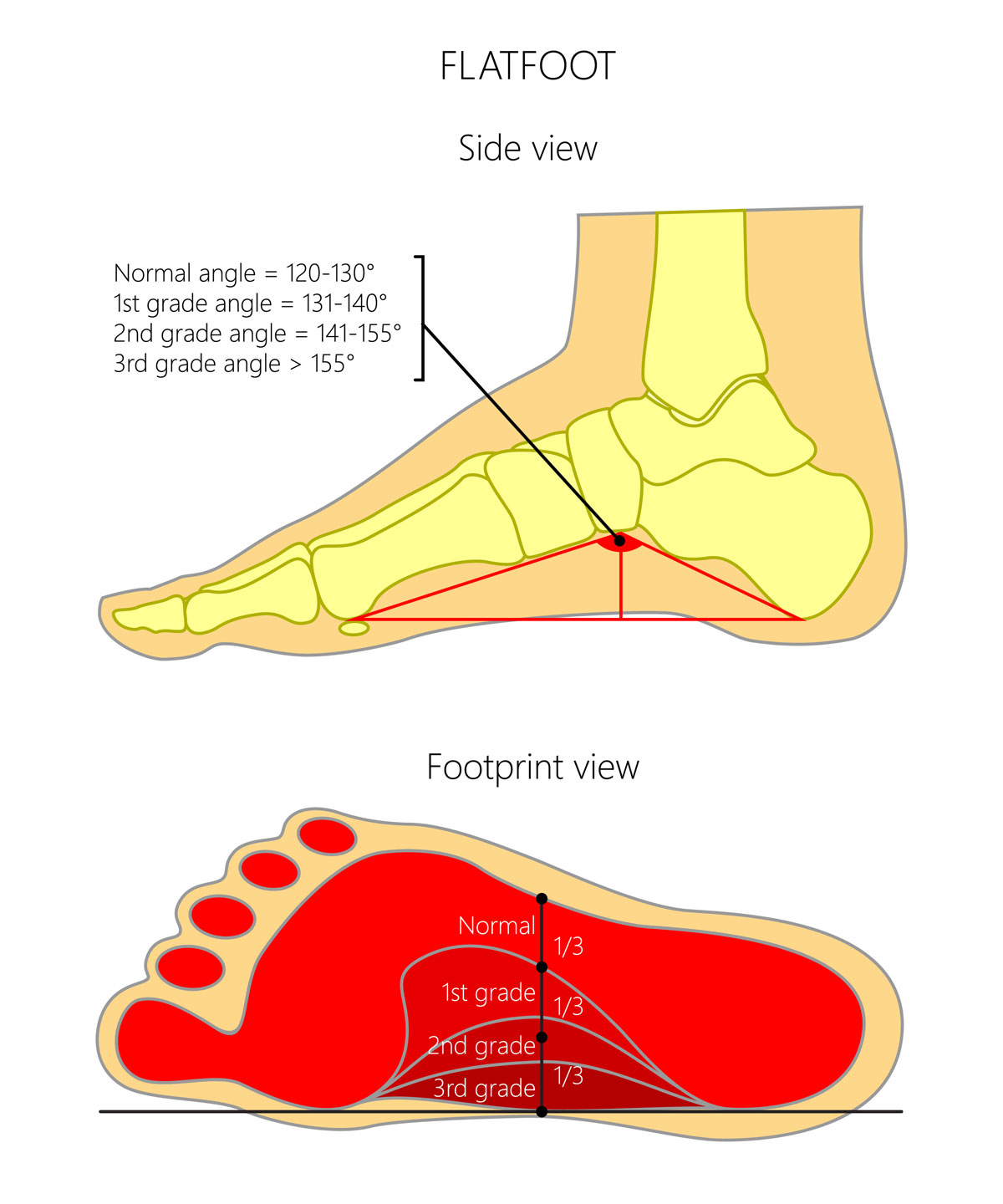
Depending on whether the deformity can be manually reduced, flatfoot can be classified as:
- Flexible – the arch can be restored by moving the foot by hand.
- Rigid – the arch cannot be restored manually
A deficiency of the plantar arch may have various causes:
- Congenital abnormalities of the foot bones
- Trauma to the foot or ankle
- Weakness of the muscles supporting the arch
- Neurological disorders
- Connective tissue disorders
How Is Flatfoot Diagnosed?
In children, flatfoot is almost always asymptomatic.
Some mild, non-specific signs may include fatigue, cramps, or occasional limping. Rarely, a child may complain of pain on the inside of the foot arch, which can indicate posterior tibial tendon strain.
A medical evaluation is recommended when:
- The feet or other parts of the lower limb are painful
- Shoes wear out quickly on the inner edge
- The arch is completely absent
Diagnosis is often based simply on a physical examination and medical history.
A doctor’s visit is recommended if:
- Feet or legs hurt
- The arch is completely absent
- Shoes wear unevenly
Diagnosis usually requires only a physical exam. X-rays or other imaging tests are performed if the pain is significant.
Treatment of Flatfoot
In reality, only a small percentage of patients with flatfoot experience pain. However, several studies have shown that children with flatfoot—especially those with valgus–pronated heels—are more likely to develop secondary conditions in adulthood, such as ankle osteoarthritis and hallux valgus (bunions). Surgery, in these cases, is often a preventive measure.
Non-surgical (conservative) treatments may include:
- Use of orthotic insoles
- Stretching exercises for the calf muscles
- Dietary programs for weight reduction in overweight patients
The Riva Method for Treating Flatfoot
The Riva Method can, within 3–4 months, produce significant functional and structural modeling of the foot. This can completely resolve mild to moderate flatfoot or significantly improve severe cases.
The Riva Method is also essential for preparing the foot for surgery and achieving the best possible functional and structural recovery after surgery.
Surgical Treatments
Used in select cases, often to prevent future problems like arthritis or bunions.
- Calcagno-stop
Through a small incision, a screw is inserted into the talus bone. The end of the screw, which is slightly larger (often spherical), is positioned in the sinus tarsi, where it blocks excessive pronation of the calcaneus, helping to restore the arch.
After surgery, two braces are used, allowing the child to stand after 2–3 days and walk with two crutches. After about 3 weeks, the braces are removed, and the child can walk freely. The screws are kept in place for approximately 18 months, allowing the body time to correct the foot and establish a new motor pattern. After this period, they are removed during a follow-up procedure.
2. Endothesis
Through a small incision, a metallic or absorbable implant is placed inside the sinus tarsi, counteracting pronation of the calcaneus and restoring the arch.
After surgery, plaster boots are applied. If only one foot is operated on, the child can walk on the healthy leg with crutches. If both feet are operated on, the child remains in bed until the casts are removed, approximately after 1 month. The implants are removed after 2 years—unless absorbable.