
What is it?
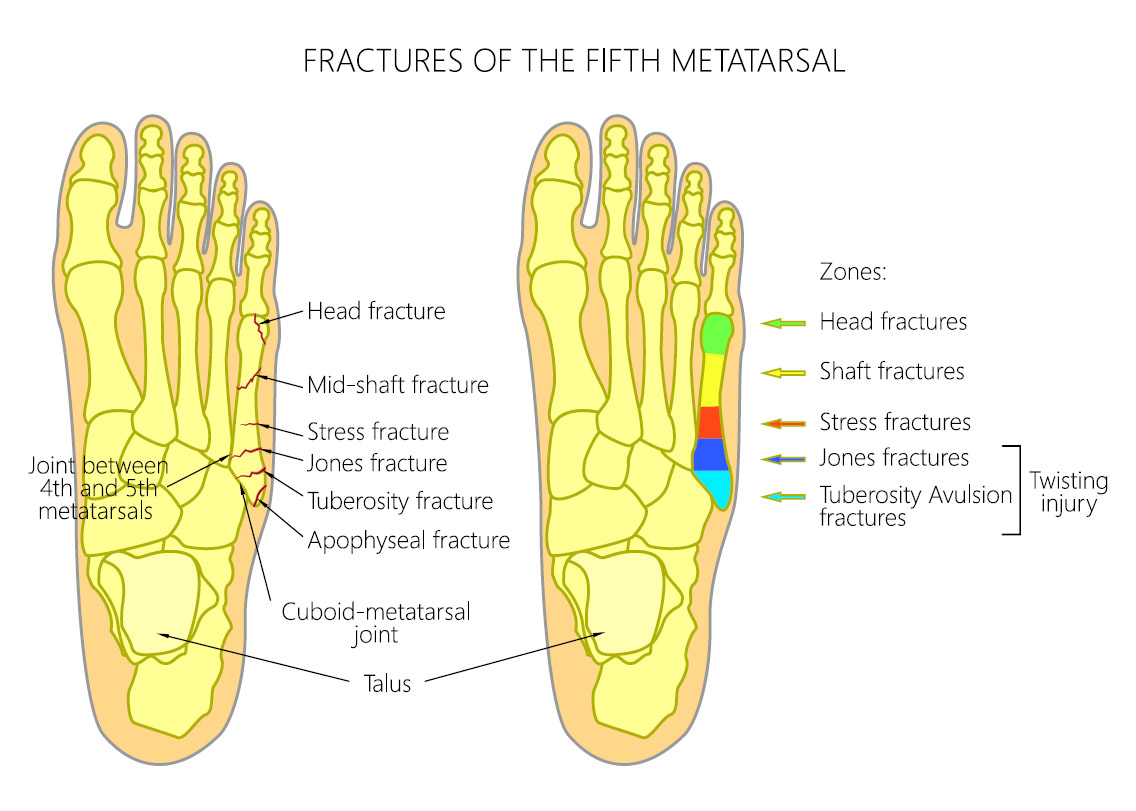
A Jones fracture affects the proximal portion of the 5th metatarsal bone, at the metaphyseal–diaphyseal junction. The injury is named after the English surgeon Sir Robert Jones, who first described it after sustaining the fracture while dancing.
The fracture typically occurs about 1.5 cm distal to the tuberosity of the 5th metatarsal. This region already has limited blood supply, and the fracture further disrupts the intramedullary arteries that nourish the bone, creating a situation of poor vascularization that slows or prevents proper healing.
When a Jones fracture occurs, the tendons of the peroneus brevis and peroneus tertius exert divergent traction on the fracture fragments—brevis inserting on the tuberosity, tertius on the shaft distal to the fracture line. This opposing pull further complicates the healing process.
Causes of 5th Metatarsal Fractures
Depending on the cause, three main types of fractures can be distinguished:
- Traumatic fracture
Caused by a sudden direct impact to the 5th metatarsal. Common in soccer, basketball, and combat sports (e.g., karate, kickboxing). - Avulsion fracture
The most frequent type. Occurs during an ankle inversion sprain when a small bone fragment is pulled away by the sudden traction of the peroneus brevis tendon at its insertion on the tuberosity. The avulsion results from reflex contraction of the muscle attempting to limit the severity of the sprain. - Stress fracture
Bones are living structures constantly remodeled by the opposing activity of osteoblasts (formation) and osteoclasts (resorption). Excessive mechanical stress (e.g., repeated impacts during running or jumping, especially when the foot lands on its lateral edge) increases bone resorption in overloaded zones. This leads to microdamage accumulation and eventually a fracture without acute trauma, caused by progressive weakening of the bone structure.
Classification of Proximal 5th Metatarsal Fractures
Three main fracture patterns can be identified:
- Avulsion fracture of the tuberosity
- Jones fracture
- Stress fracture
Jones fractures extend toward the articulation between the 4th and 5th metatarsals. Stress fractures typically occur distal to this joint.

Diagnosis
A 5th metatarsal fracture is always accompanied by pain, typically following trauma.
Diagnosis is confirmed with X-rays in anteroposterior, lateral, and oblique views. In cases of suspected stress fracture, CT or MRI may be required to detect bone marrow edema and fracture lines not visible on plain radiographs.
Conservative treatment (nondisplaced fractures):
Immobilization with a below-the-knee cast (keeping the foot slightly supinated to relax the peroneal tendons). More commonly today, Walker boots are used. These braces restrict movement, promote healing, and allow easier hygiene. However, they must be worn continuously, including at night. Immobilization typically lasts 3–5 weeks. Extending beyond this period increases the risk of disuse osteoporosis.
Surgical treatment (displaced fractures):
If the fragments are significantly separated, surgery is required to achieve reduction and stabilization, usually with a screw or plate fixation. Recovery times depend on the severity and surgical technique.
Preventive Role of the Riva Method
Regardless of the treatment chosen, rehabilitation is critical to prevent recurrence. If the underlying causes are not corrected, repeat fractures are likely.
A crucial yet often overlooked factor is the structural condition of the foot. Lifestyle in developed countries leads to progressive deterioration of foot strength and function, with fragility in muscles, ligaments, tendons, and bones. Among young people, foot development often remains incomplete, both anatomically and functionally.
The most important causal factor is the “flight phase” alignment of the foot. Instead of maintaining a neutral position while airborne, the foot often assumes an inverted posture due to weak pronator muscles and relatively stronger supinators. This predisposes the foot to inversion sprains and concentrates mechanical stress on the 5th metatarsal during landing.
The Riva Method, using High-Frequency Proprioceptive Training (HPT) on the Delos system, acts on three levels:
- Pre-impact phase
- Restores neutral foot alignment during the flight phase, preventing stress from concentrating on the 5th metatarsal.
- Impact phase
- Minimizes the mechanical forces transmitted to foot structures.
- Increases the foot’s structural resilience, improving its ability to absorb stress without injury.
- Post-fracture rehabilitation
- Once weight-bearing is possible, the Riva Method can be applied.
- Through tens of thousands of controllable mechanical stimulations, it restores tendons, ligaments, joint capsules, and bones.
A systematic program of 3–4 months is required to achieve lasting results otherwise unattainable. Patients typically perceive meaningful improvements within the first few weeks, which become progressively more significant over time.s that will become increasingly important over time.